The Many Masks of Fibrous Dysplasia: A Radiologist’s Guide to Avoiding Missteps
Fibrous dysplasia (FD) is a benign fibro-osseous disorder with highly variable imaging appearances that can mimic multiple bone pathologies. Recognizing its spectrum is essential to avoid misdiagnosis and unnecessary invasive procedures.
Fibrous dysplasia accounts for approximately 2.5–5% of benign bone lesions and results from postzygotic mutations in the GNAS gene, leading to replacement of normal bone with immature fibro-osseous tissue. The timing of mutation influences disease extent, ranging from localized monostotic lesions to widespread polyostotic involvement or syndromic forms.
FD is classically divided into monostotic (58–80%), polyostotic (20–42%), and syndromic forms (3 12%), including McCune–Albright syndrome and Mazabraud syndrome. In polyostotic forms, lesions often follow a unilateral and dermatomal distribution, reflecting embryological migration patterns. Commonly affected sites include the femur, craniofacial skeleton, tibia, and pelvis.
Clinically, monostotic FD is often asymptomatic and incidentally discovered, whereas polyostotic forms are usually diagnosed in childhood due to fractures, deformities, or growth disturbances. Craniofacial involvement may result in compressive symptoms or cosmetic deformities such as leontiasis ossea or mandibular prognathism.
Radiological presentation is highly variable and depends on lesion composition and location. Plain radiography remains the cornerstone of diagnosis, typically demonstrating an intramedullary lesion with a characteristic ground-glass matrix, bone expansion, and endosteal scalloping. However, atypical features such as cystic changes, mixed lytic-sclerotic patterns, or thick sclerotic rims may occur and create diagnostic uncertainty.
In long bones, lesions are predominantly diaphyseal, while craniofacial involvement often shows mixed patterns, ranging from ground-glass opacity to dense sclerosis, particularly at the skull base. Rib lesions typically present as fusiform expansions and are often incidental findings, whereas spinal involvement is rare but more frequent in polyostotic disease.
CT plays a complementary role, providing precise delineation of lesion margins and cortical integrity. The presence of a sclerotic peripheral rim, known as the “rind sign,” supports a benign, slow-growing process and is particularly helpful in craniofacial lesions.
In contrast, MRI has limited specificity, as signal characteristics vary according to fibrous content and mineralization, often mimicking aggressive or neoplastic lesions. Typically, FD lesions are hypointense on T1-weighted images and show variable T2 signal with minimal enhancement. Therefore, MRI should be reserved for cases with suspected complications or soft tissue involvement, rather than routine evaluation.
Bone scintigraphy may demonstrate increased tracer uptake and is useful in assessing the extent of polyostotic disease.
The main challenge in FD lies in its differential diagnosis. Conditions such as ossifying fibroma, non ossifying fibroma, osteofibrous dysplasia, enchondroma, chondrosarcoma, giant cell tumor, osteomyelitis, Paget’s disease, osteosarcoma, aneurysmal bone cyst, and intraosseous meningioma may present overlapping imaging features. However, FD is typically characterized by a smoothly expansile intramedullary lesion with a ground-glass matrix and absence of aggressive features, which helps distinguish it from malignant or inflammatory processes.
Malignant transformation is rare (<1%) but occurs more frequently in polyostotic forms, highlighting the importance of clinical and imaging follow-up in selected cases.
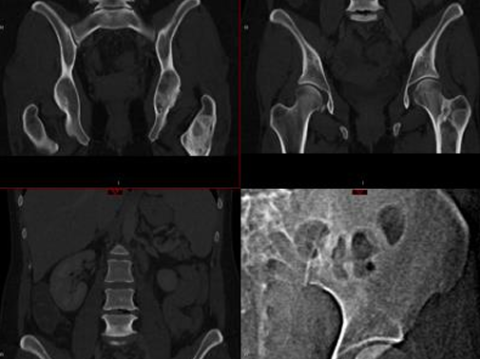
Polyostotic Fibrous Dysplasia of the left iliac bone and femur demonstrates a ground-glass appearance and cystic features, surrounded by thick sclerotic rims.
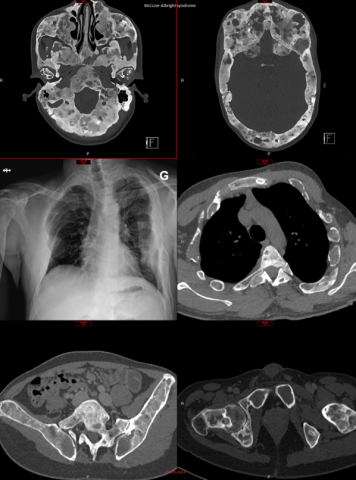
McCune–Albright syndrome
Conclusion
Fibrous dysplasia presents with a broad spectrum of imaging appearances that may lead to diagnostic pitfalls. A careful approach integrating lesion location, distribution, and characteristic imaging features—particularly on radiographs and CT—allows confident diagnosis. Avoiding routine MRI in typical cases is crucial to prevent unnecessary investigations and biopsies.